Weak Quads and Adductors: Femoral Nerve Compression
Five clues that the cause of your weak thigh muscles is Femoral nerve compression:
you don’t have the strength to lift one knee easily;
despite exercise, muscles in one thigh are weaker and maybe appear smaller than in the other thigh;
occasionally your leg “gives out;”
your thigh feels numb;
you have back pain.
Femoral Nerve Location
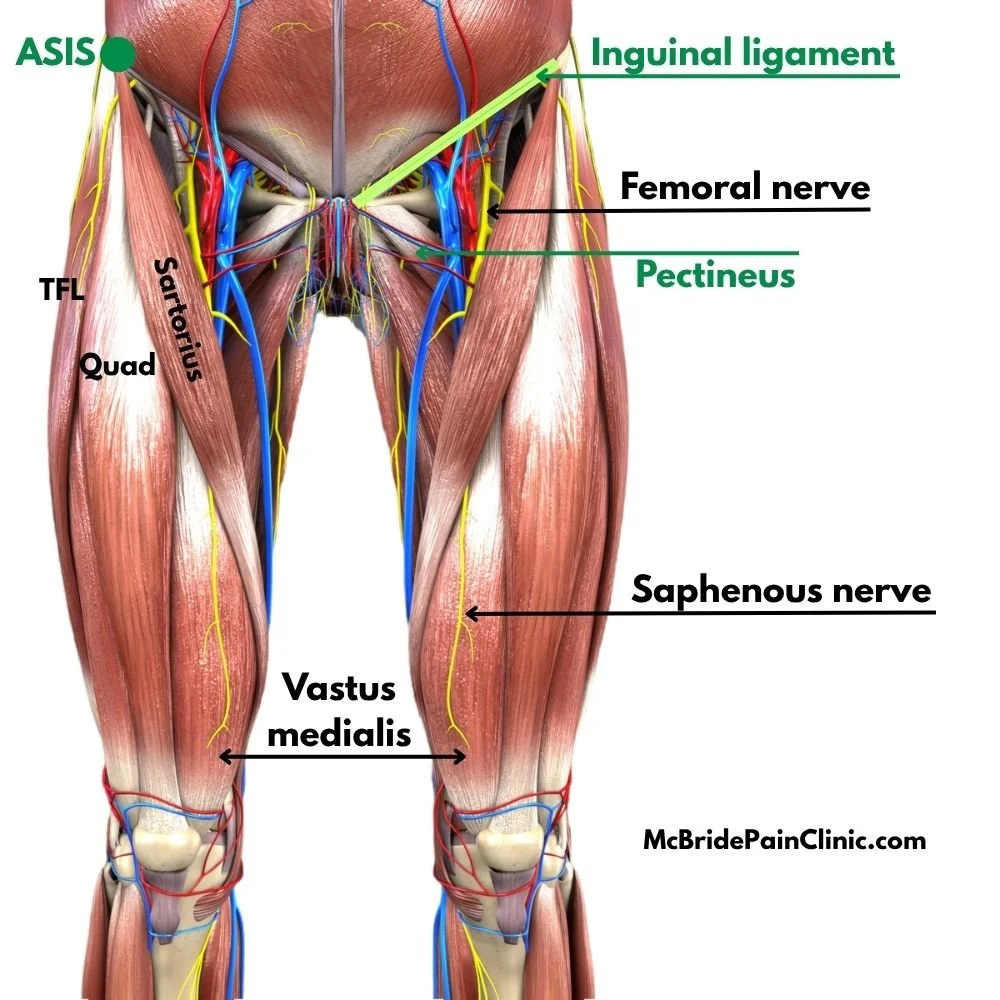
The Femoral nerve originates at the lumbar vertebrae and travels through the pelvis deep to the Psoas major muscle. It branches to innervate the Iliacus and Pectineus muscles, then passes under the Inguinal ligament to the thigh. In the image below, see that the nerve is adjacent to the Femoral artery (red) and Femoral vein (blue), important for leg blood supply.
As the nerve travels down the leg, the name changes to Saphenous nerve. It innervates the medial muscles of the leg and foot. When the Vastus medialis is damaged or too tightly contracted, thereby compressing the Saphenous nerve, people may experience severe “knee” pain.
Function
The Femoral nerve and its branches activate these muscles of the anterior thigh:
Quadriceps femoris (Quad)
Pectineus
Sartorius
Vastus medialis
Causes of Femoral Nerve Dysfunction
Muscle damage. When the Femoral nerve is compressed along its path either by a contracted Psoas major in the pelvis, or by a damaged thigh muscle, the signal to the muscles beyond that point is cut.
Surgery. Hip replacement, inguinal hernia repair, and cesareans can damage nerves and muscles in the pelvis.
Here’s another way to look at it. When you cut the electrical wire to a piece of equipment, the power is interrupted. No signal. The equipment does not work. Similarly, when a muscle compresses a nerve, or the nerve is damaged from surgery, there is little or no signal to the muscles and they do not work.
The result is thigh muscle weakness, numbness and eventually muscle atrophy. The leg can “give out,” causing falls.
What can cause muscle to tighten?
Muscle damage can be cumulative. For example, you may play an intensive sport. Over time, injuries accumulate around the original injury. Eventually muscle knots create severe enough muscle contraction to compress the nerves traveling through them. Below are typical causes of muscle damage.
Excessive exercise.
Heavy lifting.
Fall, accident, or other impact trauma.
Surgery / scar tissue.
Deep tissue massage that tears muscle fibers.
Solution: Release the muscle tension and/or scar tissue compressing the nerve.
Case 1: Woman with Right Hip Replacement
Last winter a friend from another city had right hip replacement surgery. When we met up at a weekend event the following summer, she told me she still could not lift her leg to 90 degrees, despite physio. Her right lumbar area was sore. Her surgeon wanted to schedule surgery to "strip the scar tissue off the bone."
I had first treated her right Psoas major at the event the previous year, at least six months before her hip replacement surgery. I’d found an ilium anterior rotation caused by right psoas damage. (Over time, her chronic right ilium anterior rotation had contributed to hip osteoartritis because the femur head could not sit correctly in the pelvis socket.) This second time, I knew what to look for.
Although her surgeon had made an incision on the right upper lateral thigh, scar tissue was not the issue. A hard lump of muscle had again formed in her right Psoas major just superior to the inguinal ligament. It was crushing the deep Femoral nerve. I suspect the trauma of surgery triggered the vulnerable Psoas muscle to contract.
[A raised lump of muscle at the Inguinal ligament can be constraining an inguinal hernia. To be safe, I’ve asked clients to have an ultrasound to determine whether that muscle "lump" is protecting an inguinal hernia. If the scan report confirms an inguinal hernia, I do not touch the Psoas major.]
After 30 minutes of targeted treatment through clothing on the psoas lump to "melt" it and take the pressure off the nerve, she regained some strength in the leg. The release of psoas muscle tension also corrected her right ilium anterior rotation. With power restored to the quad muscle, exercise will rebuild the atrophied anterior leg muscles.
I taught both her and her husband my muscle release technique in order to keep the right Psoas tightness under control. "As soon as your back starts to hurt, that's the signal to release the Psoas muscle at the groin,” I told them. “Because that contracted Psoas is what is causing the ilium anterior rotation, femoral nerve impingement, and weak thigh muscles." She is thinking about cancelling the surgery.
Case 2: Male, Early 40s, Martial Arts Practitioner
This fit male had “pulled his left groin muscle.” I palpated to discover a very tight left Iliopsoas to the point that it was blocking lymph flow, as evidenced by swelling in the region of the inguinal ligament. In addition, his Sartorius, quad, and Tensor fasciae latae (TFL) were like a concrete slab where they all attached to the pelvis at the left ASIS. That is, those muscle fibers were locked in contraction and not able to do work. All his adductors were tight. Combined, extreme muscle tension pulled his left ilium into an anterior rotation. This caused the left hamstrings to stretch. He had significant damage in his right lumbar muscles.
I include this case to illustrate that femoral nerve compression can be caused by thigh muscle damage rather than, or in combo with, Psoas major damage.
Case 3: Senior Hiker 3 Years After Knee Replacement
A hiker in her mid 70s had endured two tendon transplants in her 20s, then an orthoscopy and a full knee replacement three years before seeing me. When I palpated her left upper thigh, my fingers dropped into a crevasse. Her left Pectineus seemed to have atrophied to a mere sliver of its normal size. As in Case 2, her left Sartorius and TFL at the ASIS were very tight. Her left knee was noticably swollen. As well, she had damage in her right lumbar and abdominal muscles.
This out-of-town client booked a total of four sessions over a period of three months. Besides addressing muscle damage in her right lumbar and left calf, I released the muscles overlaying the femoral nerve, including the Psoas major and tight thigh muscles, addressed the painful Vastus medialis, and released knots in a stretched left hamstring. By the fourth session the Pectineus had regenerated to normal size!
Author Bio: Madeline McBride, M.A.Sc., P. Eng., studied civil engineering at Queen’s University and the University of Waterloo. Those mechanics and structural design courses inform her ability to assess in 3D, and problem-solve how muscle tension pulls a client’s skeletal structure out of alignment. Her engineering background, combined with several manual training modalities, produced this Canadian expert in restoring pelvis, jaw and spinal alignment. Madeline is able to resolve recent ilium rotations and related back, hip, knee and neck pain within one to four sessions. Long-standing, complex issues may take longer due to the body’s entrained compensation. Madeline teaches Biomechanics of Back, Hip, and Knee Pain in-person and on-line. Register for a workshop or read her blog posts at www.McBridePainClinic.com