Jaw and Pelvis Misalignment Case

Jaw & Pelvis Misalignment Case
I had a middle-aged client who came for chronic right temporomandibular joint (TMJ) pain. But assessment revealed that she had a double-ender issue – a misaligned jaw as well as a misaligned pelvis. Note that she did not report any back pain or sciatica. Her concern was significant right TMJ pain.
The treatment description below is primarily for the benefit of my students, as a reference. It is a complex case, but illustrates how important it is to treat both the jaw and pelvis alignments.
However, other readers may identify with the double-ender situation I describe. Reader, if you’re struggling to find help for jaw and/or back pain, suggest to your favourite manual therapist that s/he take my workshops!
So where does a therapist start in this situation?
Align the pelvis.
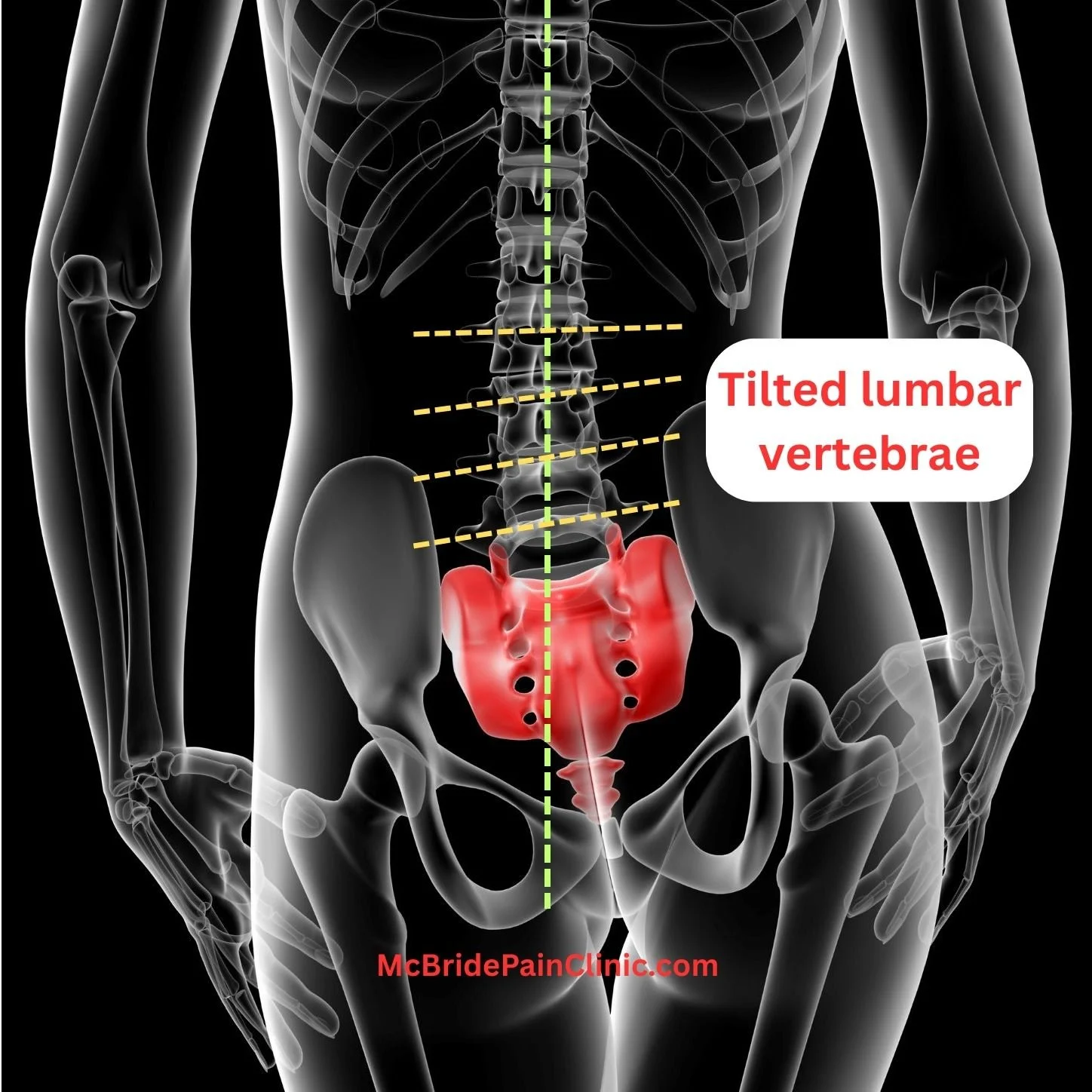
Why? Because if muscles in the pelvis and legs are damaged, causing ilium rotations and non-level iliac crests, it’s impossible for the other end of the spine to be aligned. The cervical spine vertebra and skull at the other end of the spine will also be tilted. The mandible will be misaligned, regardless of the condition of the mastication muscles.
Madeline’s Rule #1: Restore pelvis alignment first.
Until muscle damage affecting the pelvis is addressed, and pelvis alignment restored, there is no point in treating the jaw.
Madeline’s Rule #2: Find the muscle damage and Fix it.
Stretching a damaged muscle is a recipe for more damage. The better approach is to find the muscle strain, knot, or scar tissue, and release the locked fibers so the body can heal them. That permanently eliminates the source of tension.
Note: To keep it simple, I use the term “ilium rotation” rather than “innominate rotation” in this post.
CLIENT ASSESSMENT
Right iliac crest high one finger width, standing and seated. Her right sacroiliac joint (SIJ) was immobile (locked).
Neck rotation: 50 deg from center to right, 48 degrees from center to left.
Front Line Test (variation of Iliopsoas Test): both legs weak.
TREATMENT
1. Treat ilium Rotations
Both sides of the body failed the Front Line Test. First I palpated anterior thigh muscles, discovering a very hard and bulging right Tensor facia latae (TFL). It attaches to the ASIS. When contracted, the TFL has the tensile force to anteriorly rotate the right ilium. [We will see in the re-assessment why the right ilium was initially net posteriorly rotated (i.e., one finger high on right), not anteriorly rotated.]
Because of the weak Front Line Test on the left as well, I palpated for the cause of a potential left ilium anterior rotation. I discovered and treated a strained left iliopsoas. Then I turned her over, and treated a severe strain in the lumber psoas and in her obliques. That confirmed a left anterior ilium rotation.
Re-assessment: Iliac crests were two (2) fingers high on right when the client was standing and also when seated. The tight right TFL had counterbalanced tight hamstrings dragging the ilium posterior. Releasing the anterior thigh tension then made the posterior rotation worse!
Treatment, continued:
The next step was to release the very tight right hamstrings pulling the ilium into a worse posterior rotation.
Re-assessment: Then the iliac crests were even, standing and seated.
Front Line test: left moderate. Right strong.
The above treatment took an hour. But she had driven several hours to see me for her sore right jaw, so I moved on.
2. Treat Neck Muscles
Assessment: I already knew her neck rotation was problematic. The question was which muscles were causing it.
The right side of her occiput was pulled inferior. The posterior right neck muscles were extremely tight.
Treatment:
I released a very contracted right Levator scapulae. When tight, it pulls the cervical spine out of alignment.
I released very contracted right Splenius capitis and Semispinalis capitis from the upper back to the occiput and Mastoid process of the Temporal bone.
Moving to the anterior muscles of the neck, I treated a very contracted Digastric muscle between the Hyoid bone and the right Mastoid process.
At some point in her life she’d probably had whiplash. Recall her pain was in the right TM joint. Her Mandible (lower jaw) was being pulled inferior by the Digastric muscle, and also was being dragged to the left by a tight Temporalis, as I soon discovered.
Re-assessment: Left occiput now low.
Treatment: Released tension in the left SCM and throat muscles.
Re-assessment: Occiput even.
3. Treat Mastication Muscles
I discovered and treated a strain in her left Masseter.
Her left Temporalis was tight and bulging (indicating damage) at its attachment to the mandible. I released tension throughout the Temporalis. I was surprised she did not have a headache as her Trigeminal nerve would have been quite compressed.
Then I released the right Lateral pterygoid, the SCM and Splenius capitis at the mastoid process - all very tight. Tension in the right Lateral pterygoid would have counterbalanced the pull of the damaged left Temporalis. In effect, the right condyle was not seated in its socket properly, causing the chronic pain.
4. Align Sphenoid Bone
After rechecking that the Occiput remained level, I aligned the Sphenoid using my own technique.
5. Final Assessments
Iliac crests were even standing and seated.
Neck rotation was slightly better.
No Mandible wobble on jaw opening and closing.
Treating the jaw muscles took another hour. The client had a double session. It’s a lot for the body. I warned her that she would be very tired the next day, the right jaw would still be sensitive, muscles take time to heal, and to stick to soft foods for a few days.
Madeline McBride, MASc., PEng, studied civil engineering at Queen’s University and the University of Waterloo. Mechanics and structural design courses underpin her knowledge of biomechanics and tensegrity. Her engineering background, combined with several manual training modalities, produced this Canadian expert in restoring pelvis, jaw and spinal alignment. Madeline is able to resolve recent ilium rotations and related back, hip, knee and neck pain within one to four sessions. Long-standing, complex issues may take longer due to the body’s entrained compensation. Madeline teaches Biomechanics of Back, Hip, and Knee Pain in-person and on-line. She teaches Jaw and Sphenoid Alignment in-person. Register for a workshop or read her blog posts at www.McBridePainClinic.com